TRACKING COVID-19 VACCINE PURCHASES ACROSS THE GLOBE
Download our vaccine purchasing data here: https://launchandscalefaster.org/COVID-19. Note that our bivalent vaccine purchasing data is up-to-date as of May 5, 2023 and our vaccine purchasing data is up-to-date as of July 1, 2022. We are not further updating the data or webpage content at this time.
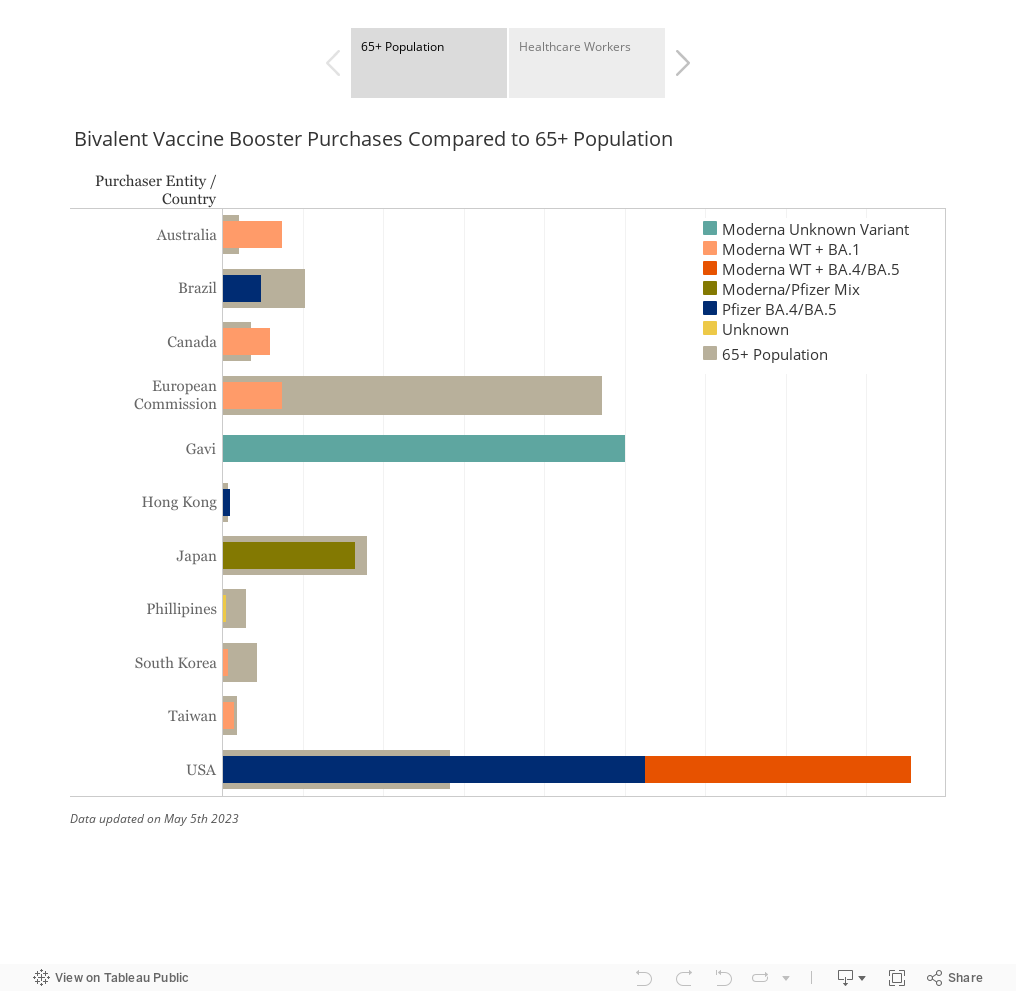
COVID-19 Bivalent Vaccine Market
COVID-19 vaccines can now be classified as monovalent (containing only the wild-type strain) or bivalent (containing both the wild-type strain and circulating variant). In response to highly transmissible variants such as omicron, Pfizer and Moderna have updated their existing vaccines to include either the original omicron strain (BA.1) or an omicron subvariant strain (BA.4/5) in addition to the wild-type strain. These new bivalent vaccines are only approved for use as booster doses, not the primary vaccination series. the hope for bivalent vaccines is that they will pave the way for development of multivalent or pan-coronavirus vaccines that provide broader protection than existing vaccines. Early clinical trial data suggest these new boosters produce higher levels of antibodies to COVID-19, yet there is concern about whether translates to clinical significance.
Currently, bivalent vaccines from Pfizer and Moderna have received provisional approval for use as boosters in a handful of countries and regions. High-income countries have purchased enough doses to vaccinate their vulnerable 65+, and the second tab shows the number of bivalent vaccine doses relative to the population of healthcare workers. Read our blog post for more details on bivalent vaccines and new vaccine technologies coming to the market.
Gavi has signed an agreement with Moderna to provide access to up to 100 million bivalent vaccine doses via the COVAX platform. However, primary vaccination coverage in low-income countries whose priorities remain on increasing primary COVID-19 vaccination may result in additional vaccine wastage. Regulatory and distribution pathways must be created and maintained to ensure these products are available everywhere. As major funding mechanisms, such as ACT-A, are transitioning from emergency response to long-term disease control, there must be renewed effort to enhance low and middle-income countries' vaccination strategies and to ensure equitable access to new vaccine technologies. For additional insight on COVID-19 vaccinations, read our COVID GAP blog.
From November 2020 to June 2022, we tracked the unprecedented number of purchases made by countries and multilateral partnerships eager to reserve COVID vaccine supply, many even before any candidates were on the market. Our visualizations and analysis from this data is available below.
We thank Linksbridge for providing access to its vaccine purchase dataset for cross-referencing purposes.
17.9 billion doses reserved
Countries have purchased vaccine doses from a wide pool of candidates to cover their populations. So far, confirmed purchases cover 11.9 billion doses, with another 6 billion doses currently under negotiation or reserved as optional expansions of existing deals.
Tab 1 shows total purchases by country, while tab 2 illustrates the timeline of these deals.
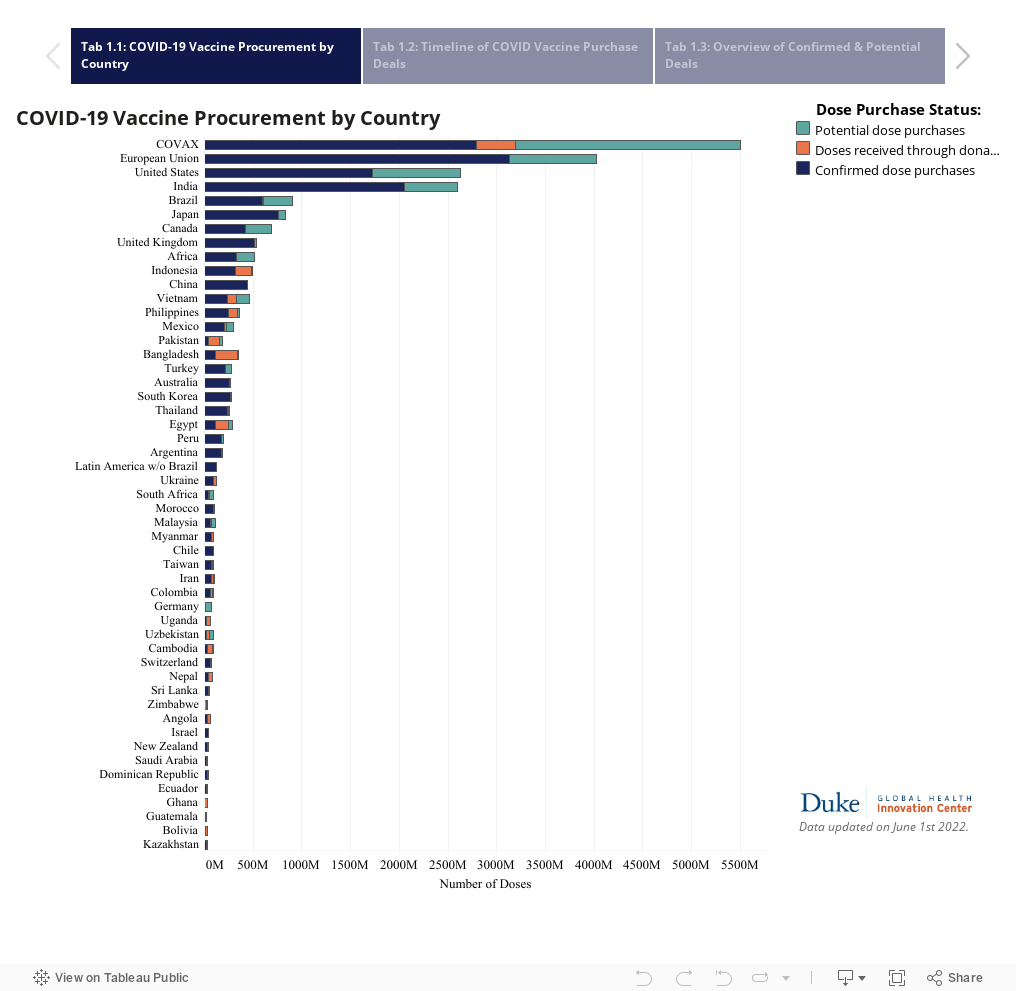
The first purchases were made in May 2020 by the US and the UK for the Oxford-AstraZeneca vaccine. These were quickly followed by a slate of purchases by high-income and some middle-income countries and, by the end of the summer 2020, the UK, EU countries, and Canada had purchased enough doses through advance market commitments to cover more than their entire populations. The first purchases for low-income countries came in January 2021, through the African Union's pooled procurement approach. Many countries in Latin America, Africa, and Asia still have not yet been able to purchase enough vaccine to cover their populations.
It is important to remember that purchase of vaccine is not the same as delivery of vaccine. For instance, despite Canada's early deals, it has received only a fraction of what it has ordered. Read our blog post for more on Canada's experience.
The data presented in the map above captures when the deals were made, not the timeline for delivery or actual vaccinations. Our data does not include vaccine purchases made by COVAX (currently at 1.6 billion doses) or the population coverage provided by COVAX to participating countries. Our data also does not include domestic supply data for Russia or China, as this information has not been made publicly available.
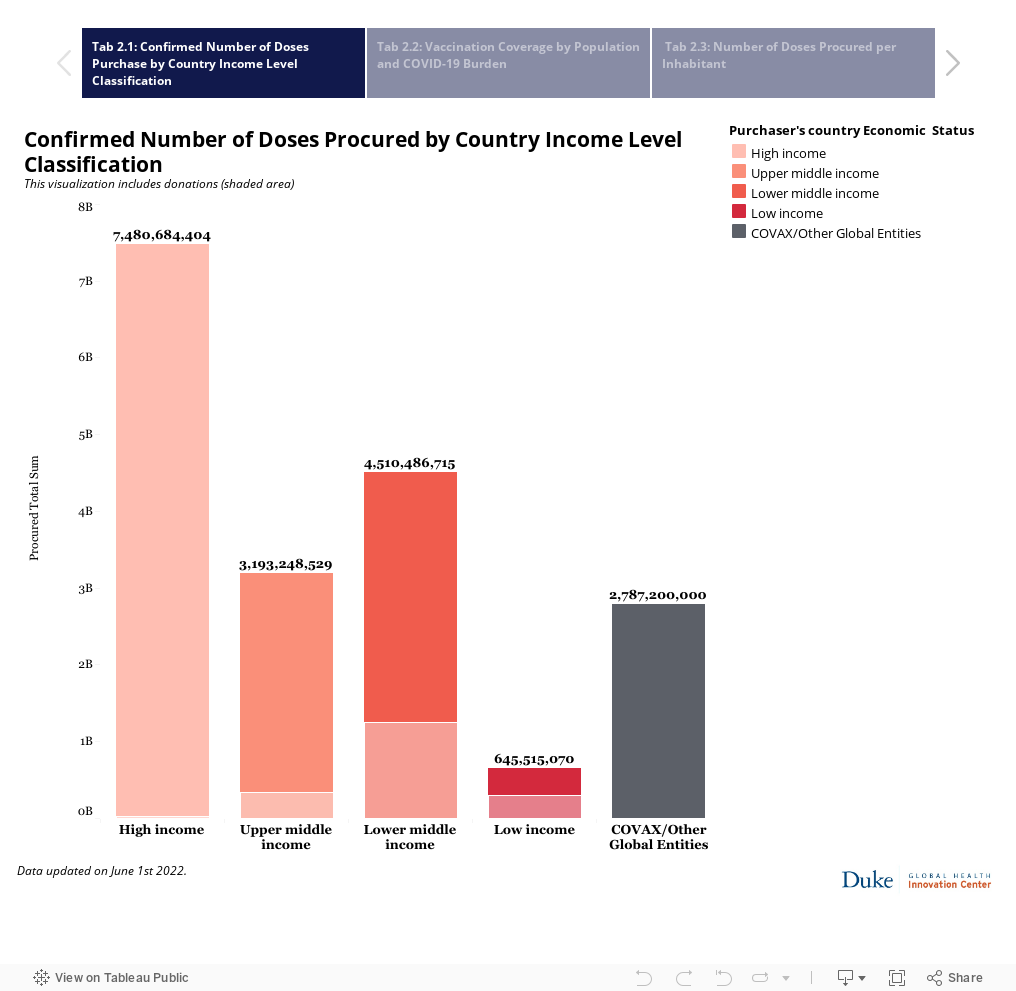
High-income countries hedged their bets while low-income countries were left out
In 2020, many high-income countries hedged their bets by purchasing enough doses to vaccinate their populations several times over, even before any candidates were approved and have continued to procure more doses of approved vaccines in 2021, in an effort to receive doses as quickly as possible. Because of global manufacturing constraints, the direct deals made by high-income (and some middle-income) countries mean that a smaller piece of the pie is available for low- and middle-income countries and for equity-focused partnerships like COVAX in 2021.
Tab 1 provides number os doses purchased by country income level. Tabs 2 and 3 show coverage by country at population and individual level, respectively.
The Role of Covax
Demand has outstripped supply for COVID-19 vaccines around the world since the first vaccines came to market. Manufacturing capacity can be expanded with targeted investment but only to an extent and it will remain a rate limiter through 2022 (See our COVID manufacturing data here).
In this context, COVAX and other alliances are critical to ensuring equitable allocation of vaccines for low- and middle-income countries (LMICs). A partnership between GAVI, the World Health Organization, and the Coalition for Epidemic Preparedness Innovations (CEPI), COVAX is a global mechanism to promote equitable distribution of vaccines, so that the pandemic can be stopped everywhere at more or less the same time.
COVAX de-risked the purchasing process for countries by investing in the development, manufacturing, and procurement of a wide portfolio of vaccines (at a time when we were not sure that any would work). Member countries buy in at their preferred level of population coverage and receive vaccines that make it through the WHO emergency approval process. Crucially, the vaccines are shared out the same time, by population level.
The vast majority of the world's population live in COVAX-participating countries, including 92 lower-income countries, referred to as AMC or funded countries, that will receive COVAX doses at 20% population coverage without charge.
COVAX aims to provide around two billion doses by the end of 2021 to protect high-risk populations around the world. However, it is far from achieving this goal. Many high-income countries funded COVAX but also preferred to take on deals, so invested early in multiple vaccines, securing a place at the front of the production line.. Forced to compete with wealthy nations for the limited number of doses coming out in 2021, COVAX has struggled to shore up sufficient supply. COVAX deliveries began in February 2021 but, shortly after, faxed significant supply shortages, in part stemming from India's export restrictions. For more on our take on the first year of COVAX, read our piece here.
In recognition that wealthy countries would soon have excess doses, COVAX developed a dose-sharing mechanism, through which COVAX takes on liability for donated doses that are then redistributed to funded (AMC) countries. France was the first country to donate vaccine doses through the COVAX dose-sharing scheme, pledging 500,000 doses to be shared by mid-June and at least 5% of their total supply through 2021. New Zealand, Spain, and other countries have also signaled that they will donate doses through COVAX.
Jostling for a place in the queue
Among high-income countries, those that were home to vaccine makers were the first to secure large advance market commitments. They invested public funds into research and development of COVID-19 vaccines and leveraged their purchasing power to make large-scale deals across a portfolio of vaccine candidates. This investment came with a caveat: they wanted to be first in line when doses rolled off the production lines.
With limited purchasing power, middle-income countries used other strategies to get to the front of the queue for advance market commitments. Countries with manufacturing capacity, such as India and Brazil, were successful in negotiating advance market commitments with leading vaccine candidates as part of manufacturing agreements.
For countries without manufacturing or vaccine development capacity, those with the infrastructure to host clinical trials, such as Peru, tried to use that as leverage to negotiate purchase deals.
Several middle-income countries, including Russia, and China, also have robust vaccine development programs and were among the first to put forward vaccine candidates and get local approvals. See graphic below and this blog post for more details on regulatory approval timelines.
India is also playing a big role in manufacturing COVID vaccines. Serum Institute of India is manufacturing the bulk of Oxford-AstraZeneca’s and Novavax’s vaccines for distribution to COVAX and LMICs, and is developing its own vaccine candidates. Bharat Biotech has also developed a vaccine, Covaxin, that is being used domestically and abroad.
Low-income countries that lack manufacturing and clinical testing capacity were largely left out of the deal-making process. Multilateral coalitions help address this gap, such as a pooled procurement approach led by the African Union and the Africa CDC, resulting in hundreds of millions of doses purchased for African countries. However, with many manufacturing countries using export restrictions to ensure that doses meet domestic needs first, low-income countries are still at the back of the line for delivery and will likely be waiting until 2022 before they are able to cover even vulnerable populations.
Tab 1 shows the number of doses purchased by country and vaccine candidates. Tab 2 shows total sales by vaccine, broken out by income status of purchasing countries. It is important to note that not all vaccines are yet approved by purchasing countries.

There is an urgent need to for wealthy countries to share excess doses and ensure manufacturers can ship both doses and needed production materials to LMICs in order to achieve vaccine equity and herd immunity in every country. Based on our analysis of the manufacturing landscape, we think that waiving intellectual property rights, such as through the proposed TRIPS waiver, is unlikely to achieve meaningful impact. Read more about our take on this issue here.
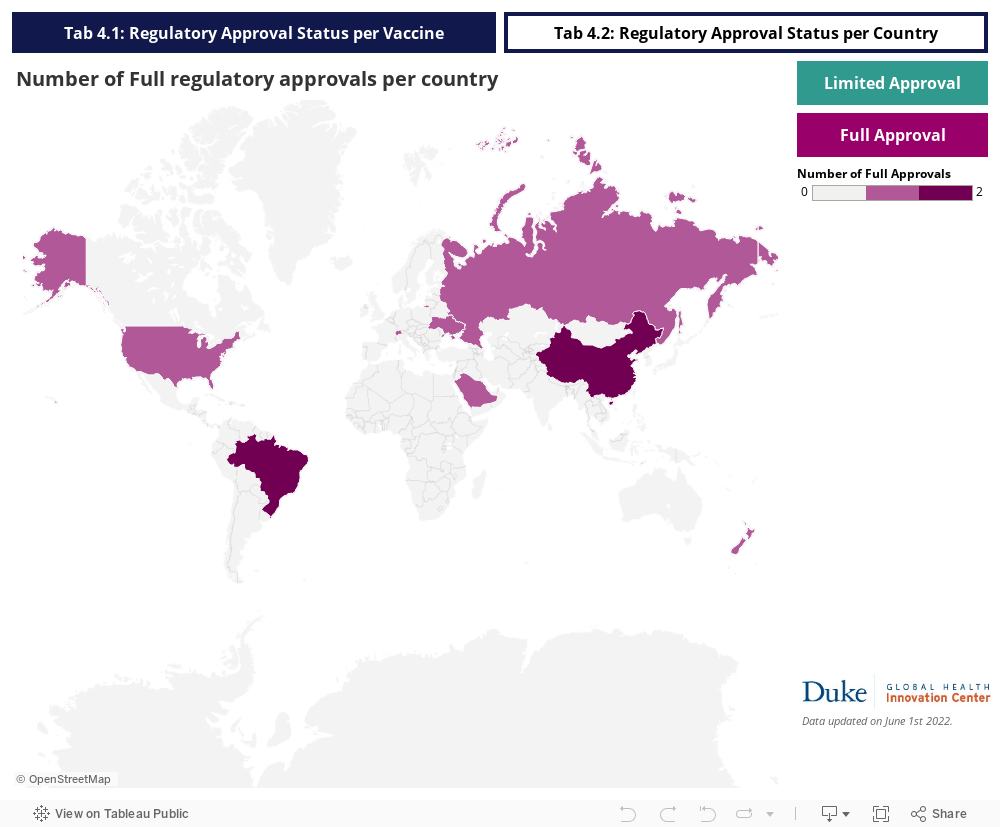
Regulatory approvals determine rollouts
Regulatory approval process and timeline differ from country to country but COVID-19 vaccines across the world have been produced and authorized for use with record speed. The first approval was announced by Russia in August 2020 for their Sputnik V vaccine, manufactured by Gamaleya Research Institute. The first vaccine to receive approval by a stringent regulatory authority was Pfizer-BioNTech in the UK (December 2020).
The data presented in this visualization captures the dates that limited (e.g. emergency use) and full regulatory approvals were granted by vaccine candidate and by country.